
Internal Radio Theranostics
The Boys Light Up
I’m showing my age a little here, but I thought the above song title from iconic 1980’s Aussie band Australian Crawl1 was an apt title for this synopsis. My aim with this piece is to provide readers with what is, at best, only a shallow dive into the current state of play in the rapidly growing medical field of internal radio theranostics. More on the connection to the song a little later, but first an introduction.
A Quick Intro
Although theranostics is a made-up fusion of two words, therapeutics and diagnostics, it has become an accepted new word, or neologism, to describe this rapidly emerging field of medical science. It seeks to be both a therapy and a diagnostic for cancer treatment.
Both functions will use the same mechanism but often contain different radioisotopes, each optimised for its targeted function. The therapy is often referred to as Targeted Internal Radiation Therapy (TIRT) although other terms are commonly used including Selective Internal Radiation Therapy (SIRT) and Brachytherapy.
Unlike the more common broad beam external radiation therapy, TIRT can more selectively target the cancer tumour with superior precision and power and less collateral damage to healthy tissue.
The ‘radio’ part of the term denotes the use of a radioactive isotope. A radioisotope (or radionuclide) is a radioactive version of a common stable element that radioactively decays over time. In simple science terms it has the same atomic number as the stable version of the element it decays to (i.e. same number of protons). However, it has a different number of neutrons (can have more or less of them). This makes the isotope unstable and subject to radioactive decay (with a half-life).
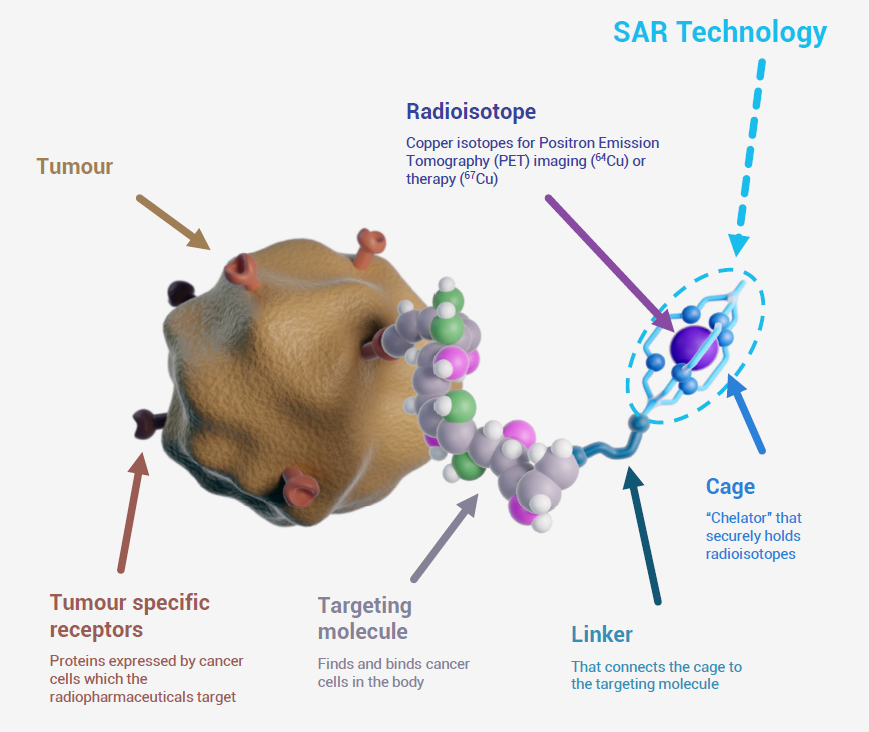
The radioisotope molecule in a radiopharmaceutical is held captive within a ‘cage’ or chelator. The cage is physically linked to a targeting molecule through a chemical chain.
The targeting molecule has properties that seek out only certain unique cancer proteins or antigens over-expressed by specific cancer tumours. Over-expression is where too many copies of certain proteins or other substances are produced, usually by cancer tumours. This helps the targeting molecule to identify the tissue as cancer and distinguish it from healthy tissue.
The targeting molecule then locks onto these proteins, a bit like a heat seeking missile. Any isotopes not finding and locking onto the receptors on cancer tumours are excreted from the body by the kidney thus causing minimal harm to healthy body tissue. Unplanned release of the isotope from its cage can cause the patient harm or toxicity. It ends up accumulating in unanticipated areas of the body and irradiating healthy tissue.
A good analogy for the isotope and the radiopharmaceutical is perhaps a fighter jet and the various ammunitions it can carry under its wings. It will load a different type of ammunition depending on the purpose of its mission. The isotope in this case is the ‘ammo’ in the TIRT that does the task required. One type of isotope (ammo) is used to seek out the cancer in the body (diagnostic) and another type used to destroy it (therapy).
Some well known examples of radioisotopes include uranium-235 (700m year half-life and decays to stable element lead-206) and carbon-14 (5,730-year half-life and decays to stable element nitrogen-14 – also used for carbon dating).
Radio therapeutics use isotopes with much shorter half-lives that deliver the bulk of their radioactivity to site over the course of hours and days. Common examples used include Gallium-68 (half-life of 68 minutes), Florine-18 (107 minutes), Lutetium-177 (6.7 days) and Copper-67 (62 hours).
The shorter half-life of these isotopes requires the doses to be prepared to order for transport and immediate use. There is no inventory in this field of medicine. Once the dose is prepared and delivered to clinician it is administered to patients via a simple injection into the blood stream.
Once attached to the tumour, the isotopes perform 2 primary functions:
- The radioactivity of the isotope can be scanned using a PET scan (similar to a CAT scan) to identify if any cancer cells are present or ‘lit up’ in the body (thus the song title). If the cancer protein or antigen is uniquely specific to that particular type of cancer, then oncologists know that all those spots lit up on the diagnostic scan are indeed cancer tumours. This helps them decide the most appropriate treatment strategy for that patient.
- The radioactive isotope, once attached to the tumour receptor, is within firing range of the tumour so that its radiation activity can burn the cancer (damage its DNA). This will help slow its progress or even potentially kill it completely (curative).
For pharmaceutical companies, the challenges of developing and commercialising new TIRTs are primarily fivefold:
- Discover or identify unique cancer receptors (proteins, enzymes, antigens etc.) specific to each different cancer that does not already exist or rarely exists outside these cancers.
Source: Clarity Pharmaceuticals
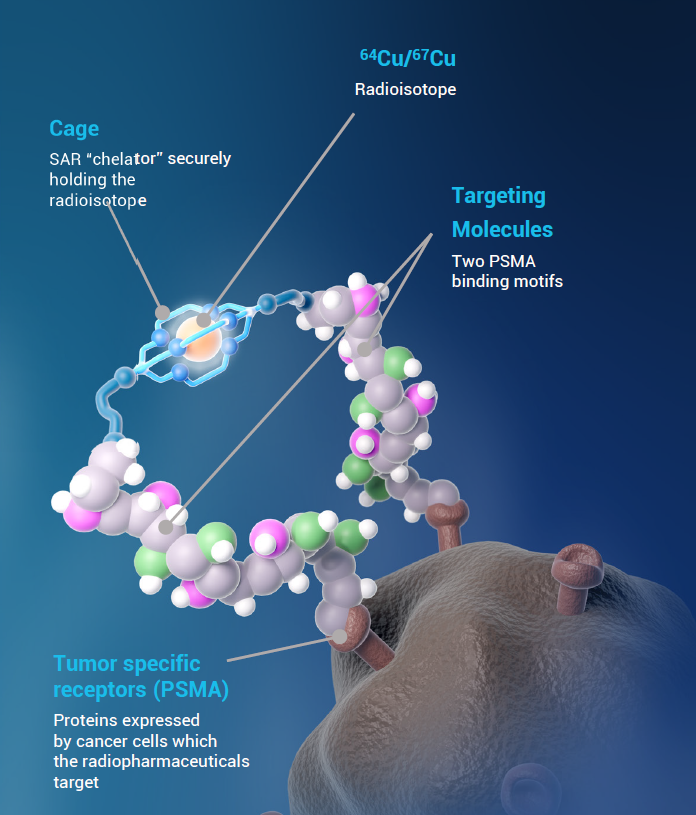
- Ascertain a targeting molecule that can be used to attach to these unique receptors and will not detach too soon during the highest intensity radiation phase of the treatment. For example, some existing small molecule drugs and antibodies can be used as targeting molecules for the tumour. Clarity Pharmaceuticals (ASX: CU6) have innovated with a dual linking mechanism that attaches to 2 separate tumour receptors (per exhibit 3). This significantly strengthens its bind to the tumour. This increases both its radioactive impact on the tumour for therapy and lengthens its scanning window (1-4 days) for diagnosis.
- Develop an isotope and associated dosing regime that will deliver an appropriate level of radiation payload (dose size) to carry out its intended function, either to light up the cancer under a PET scan (thus the connection to the song title) or to damage the cancer by irradiating it.
- The key challenge with the choice of isotope is to maximise tumour radiation whilst minimise toxicity. Side effects or ‘adverse events’ need to be kept to a minimum so as to not materially offset the benefits delivered. Radiation therapy duration and toxicity risk is amplified if the cage holding the isotope fails to contain the isotope for the most intense period of its radioactivity. Released isotopes floating around the blood stream can accumulate in healthy parts of the body and cause unintended radiation damage. Again, Clarity have innovated with a three-dimensional cage (see exhibits 2 & 3 above) that has shown an ability to hold the isotope more securely for longer, allowing for the delivery of a higher dose of targeted radiation to the tumour more safely without unintended radiation of non-cancer tissue.
- Lastly, management of the complex logistics and supply chain for theranostics. Factors to consider:
- The short half-life of the radioisotopes used. This translates to a short shelf life for the isotope and means it must be manufactured close to the patient clinic for fast delivery.
- Telix Pharmaceuticals (ASX: TLX) have innovated in this area by using commercially available Gallium-68 generators (small and relatively inexpensive devices) located at nuclear pharmacies around the US to generate the required isotopes. Its main distribution partner, Cardinal Health has one of the largest networks of generators in the US. They can produce doses of Ga-68 at short notice and close to the end customer, allowing for fast delivery to clinicians.
- The Ga-68 is itself converted by the generators from Germanium-68 (sourced from a nuclear reactor). Ga-68 can also be produced without a nuclear reactor by using a cyclotron (much larger than a generator) to bombard Zinc-68 with protons. This eliminates the risk of supply from nuclear reactors (see next point below).
- Supply chain challenges regarding access to the required radio isotopes. Much of the source material for generating medical isotopes is produced by aging nuclear reactors. These are becoming increasingly unreliable and are impacting on the security of supply to patients.
- Clarity Pharmaceuticals (ASX: CU6) has an exclusive US partner (NorthStar) that uses a device called a Rhodotron. These large machines are electron beam accelerators that produce radioisotopes through a non- uranium based, environmentally friendly process. Thus, for Clarity, Zinc-68 is transformed into Copper-67 in a Rhodotron without the need for material sourced from a nuclear reactor.
- The short half-life of the radioisotopes used. This translates to a short shelf life for the isotope and means it must be manufactured close to the patient clinic for fast delivery.
Traditional Radiation Therapy
The other much more common form of radiation therapy is external beam radiation. It has been around for a long time and directs high-energy radiation beams at the cancer from a machine outside the body.
A linear accelerator is used to deliver the radiation. It is precisely shaped into beams to target the cancer cells while hopefully minimising damage to surrounding healthy tissue.
The biggest downside of external beam radiation therapy (EBRT) is the unintended damage to healthy tissue. This is particularly relevant for healthy body tissue adjacent to or in between the external radiation source and the cancer. Other common side effects include fatigue, hair loss, nausea, dry mouth and vomiting. Less common but more severe side effects include adjacent organ damage, lymphedema and secondary cancers caused by wayward radiation.
Patients are also weighed down with a heavier schedule of treatments, usually daily for several weeks. It may also require significant travel by the patient to attend specialist EBRT treatment centres. All this can be very disruptive and burdensome for patients and their families.
In contrast, the biggest upside of modern theranostics is its ability to both precisely target the tumour for radiation whilst minimising ‘off-target’ damage and concurrently diagnose the cancer using a PET scan. Treatment is also much simpler (intravenous injection for oncology or inhalation for respiratory) and is often much shorter in duration than broad beam radiation (2-5 doses over a few weeks).
Not Our First Rodeo
In a past small cap life, the Eiger team were investors in an early pioneer of internal radio-pharmaceuticals. Those funds were large shareholders in an Australian company called Sirtex Medical (ASX: SRX).
It had developed a very early form of targeted internal radiotherapy, called SIR-Spheres.
A single dose of SIR-Spheres contained millions of micro resin beads (spheres), each coated with a beta-emitting radioisotope, Yttrium-90 that was sourced from a nuclear reactor such as the ANSTO Lucas Heights reactor on the outskirts of Sydney.

Treatment required a dose of these radioactive micro-beads to be directly injected into a cancer-burdened liver. Unlike modern radiotheranostics, it had no ability to self-seek out the cancer receptors so could not be administered with a simple intravenous injection.
The procedure required a catheter to be inserted into the femoral artery and then guided into the liver’s vascular system. It was carried out by an interventional radiologist with the aid of diagnostic imaging.

This was not a simple procedure, as we observed on a visit to St Vincent’s Hospital in 2011 (we had to wear lead- shielded vests – I’m the one on the right in green – Stephen is on left in the fetching leopard skin outfit). Any miscalculation in guiding the catheter to the correct location could cause severe and very painful intestinal ulcerations (radiation burns) to the patient from the misdirected radiation.
With a half-life of about 64 hours, the SIR-spheres would embolise in the tiny capillaries that fed blood supply to the liver tumour. Over the course of a week or two they would irradiate the cancer cells.
Unlike modern theranostics, SIR-Spheres had no diagnostic function, only therapeutic.
SIR-Spheres were able to deliver some patient life extension by halting, shrinking or even killing the liver cancer tumour. SIR-Spheres shared the benefits of TIRT being the minimised radiation harm to adjacent or ‘off-target’ healthy tissue and the delivery of ‘hotter’ radiotherapy directly to the cancer without the more severe side effects of broad beam external radiation.
They were not used as a first line therapy (i.e. on initial diagnosis). Usage was mainly consigned to what was euphemistically termed ‘salvage’ therapy (i.e. last roll of the dice after trying everything else and failing). Expectations were thus very low so any improvement in quality adjusted patient life extension was very welcome.
Sirtex was a terrific (if somewhat volatile) investment for our clients over the course of 2011 to 2018, rising from around $5 per share to around $30 when China Grand Pharma bid for the company.
Radio Theranostics are now ‘Hot’ Assets
As can be seen from our Sirtex experience, the science of TIRT has come a long way over the past decade. Surprisingly, Australian companies continue to be at the leading edge of this field with a number of prominent and very promising ASX listed companies at the vanguard.
The aforementioned examples of Telix Pharmaceuticals (with a market cap of >$6b, the largest company in the Small Ords index and next likely candidate for promotion to the ASX mid caps) and Clarity Pharmaceuticals (has very promising copper based IP and also has a large market cap of >$1.5b) are the leaders in this field. Other much smaller names include Cyclopharm and Radiopharm Theranostics.
The rapid emergence of this new field of medical science has coincided with increased attention from the large global pharma companies. They clearly see the considerable revenue potential of radio theranostics for the treatment of cancer. However, they also recognise the risk that it fundamentally changes the current standard of care best practice treatment of the disease. A do- nothing strategy could also represent a risk to any legacy cancer product revenues they retain. Theranostics thus represent both an opportunity cost and real cost of doing nothing.
We believe that for these reasons large global pharma wants to actively participate. Acquisitions in this space have increased materially in the last couple of years. Large pharma companies are on the hunt for promising acquisitions to help them grow or establish their franchises in TIRT. Recent prominent transactions include:
- Novartis acquires Mariana Oncology for US$1b + milestones in May 2024
- Eli Lilly acquires Point BioPharma for $1.4b in late 2023
- Bristol-Myers Squibb acquires Rayze Bio for US$4.1b in February 2024
- AstraZeneca acquires Fusion Pharmaceuticals for US$2.4b in late 2023.
All of these purchases were for very early-stage assets still requiring significant further R&D investment to progress them to a commercial stage. We believe more advanced therapeutic assets such as those of Telix (one of its products, Illucix, is already commercialised with fast growing revenues likely exceeding A$500m in 2024) and Clarity are in our view significantly more valuable than the recently acquired early-stage assets above.
Interestingly, in late June 2024, Lantheus (a US theranostic company with an A$8b market value and Telix’s main competitor for its Illucix prostate radio diagnostic product) announced a surprising transaction. It had acquired two (very very) early stage therapeutic and diagnostic drug candidates from Radiopharm Theranostics, an ASX listed microcap company (ASX: RAD market cap A$15m). These candidates aim to target a peptide receptor over-expressed in prostate and breast cancers.
Lantheus paid an upfront of A$3m for the two pre-clinical assets. It also subscribed for A$7.5m of Radiopharm equity at a >50% premium to the last price (with an option for the same equity again). Although small dollars for Lantheus, the question remains…why not bid for the entire company? It would certainly have been cheaper. An observer might conclude that this appears to be a panicked move to grab whatever assets they can in this mad scramble for industry positioning.
Such signs of desperation combined with other recent larger deals appears reflective of the heightened activity now underway to secure good assets in this space.
Of all the majors, Novartis is perhaps the most advanced in building itself a large franchise in targeted radiopharmaceuticals. Through a number of acquisitions, starting with Advanced Accelerator Applications (AAA) for about US$4b in 2017, it now has a number of irons in the fire. Pluvicto (therapy for PSMA- specific prostate cancer) is its major asset, generating about US$1b revenue in 2023 (up +260% from 2002).
Bayer has a small exposure to the sector through radionuclide therapies like Xofigo (radium-223 dichloride) for prostate cancer but little else.
Few other global pharma leaders have anything of significance in the field. Most are starting from scratch in building a radiopharma franchise. We expect the interest level in this rapidly growing field of medicine to continue increasing in times ahead.
Concluding Thoughts
Targeted radiotheranostics represents a major paradigm shift in cancer treatment, offering precise and effective therapeutic options for patients with various types of cancers. As research continues to advance and technologies evolve, the potential of TIRT to improve survival, enhance quality of life, and expand treatment options for cancer patients continues to grow.
Australian small cap investors have a good selection of very targeted options for investment in this specialist and fast-growing field of medicine.
Author: Victor Gomes, Principal and Portfolio Manager
- The Boys Light Up – Lyrics by James Reyne, Australian Crawl, 1980.
The song was certainly not about lighting up cancer in the human body for diagnosis and treatment. Instead, it was about lighting up cigarettes at a party (although other non G-rated interpretations can be derived from the lyrics – language warning). ↩︎
This article was written with the assistance of AI.
This material has been prepared by Eiger Capital Limited ABN 72 631 838 607 AFSL 516 751 (Eiger Capital). It is general information only and is not intended to provide you with financial advice or take into account your objectives, financial situation or needs. To the extent permitted by law, no liability is accepted for any loss or damage as a result of any reliance on this information. Any projections are based on assumptions which we believe are reasonable but are subject to change and should not be relied upon. Past performance is not a reliable indicator of future performance. Neither any particular rate of return nor capital invested are guaranteed.